




By: Prof. Dr. Seyed Saeid Zamanieh Shahri, MD and Prof. Dr. Sonia Sayyedalhosseini, MD
Disease Risk Factors:
Some factors increase the likelihood or severity of dyslipidemia; these factors do not necessarily mean a direct cause, but they are correlated with it:
• Age: As age increases, lipid composition usually shifts toward higher LDL and triglycerides and relatively lower HDL.
• Genetics and family history: The presence of familial hypercholesterolemia (FH) or early cardiac events in first-degree relatives indicates a higher predisposition to dyslipidemia.
• Obesity and metabolic syndrome: Visceral obesity has been associated with high triglycerides, low HDL, and the formation of a “small, dense LDL” pattern.
• Insulin resistance and type 2 diabetes: These conditions are linked to increased VLDL production in the liver and triglyceride accumulation in lipoproteins.
• Alcohol and certain dietary factors: High energy intake and certain dietary patterns have been reported to be associated with high triglycerides and increased VLDL.
• Underlying diseases (renal, thyroid, liver): Dysfunction of these organs can affect lipid synthesis, excretion, or distribution.
In recent epidemiological texts, in addition to the absolute levels of lipids, fluctuations in triglycerides over time have also been considered an independent risk factor for cardiac outcomes and pancreatitis.
Symptoms and Signs of the Disease:
In most individuals, hyperlipidemia remains asymptomatic for a long period, and the only way to detect it is through laboratory testing. However, in certain specific situations, the following manifestations may be observed:
• Tendinous xanthomas: Yellowish lumps on tendons (e.g., Achilles tendon) resulting from lipid deposits in connective tissue; this is particularly described in severe FH.
• Xanthelasma: Yellow spots near the eyelids reported in association with lipid disorders.
• Corneal arcus at a young age (Arcus cornealis): A whitish or grayish ring at the edge of the cornea, which in youth can indicate severe lipid disorders.
• Acute pancreatitis with very high triglycerides: In extremely high triglyceride levels, severe abdominal pain and signs of pancreatitis may occur; recent reports emphasize the relationship between hypertriglyceridemia and the severity/recurrence of pancreatitis.
Many of these signs represent late manifestations of a persistent disorder rather than early indicators of a minor increase in lipids.
Complications of the Disease:
1) Atherosclerosis and cardiovascular diseases are the main clinical consequences of hyperlipidemia, facilitating the formation of atherosclerotic plaques in the arteries. Oxidized LDL is taken up by macrophages in the vessel wall, creating ‘foam cells’; subsequently, inflammatory reactions, smooth muscle cell proliferation, and extracellular matrix deposition form the atherosclerotic plaque. This process underlies many diseases: coronary artery disease, ischemic stroke, and peripheral vascular disease.
2) Acute pancreatitis related to triglycerides
A combination of high triglycerides and severe chylomicronemia can be associated with acute pancreatitis. Recent studies have identified hypertriglyceridemia as one of the common causes of acute pancreatitis and have shown that as triglyceride levels increase, the likelihood of complications and disease severity also rises.
3) Skin and eye complications
Xanthomas, xanthelasma, and corneal arcus in youth are considered tissue manifestations of lipid accumulation and are seen with higher severity in some genetic syndromes.
4) Impact on other organs
Dyslipidemia, combined with other factors (such as high blood pressure and diabetes), can create a network of chronic damage to the small vessels in the kidneys, retina, and other tissues, although the specific role of each factor in this network is often examined in the context of multifactorial studies.
Methods of diagnosing the disease:
1) Basic lipid profile
The diagnosis of hyperlipidemia is primarily based on laboratory measurements. A “lipid profile” usually includes the following:
• Total cholesterol
• LDL (calculated or measured)
• HDL
• Triglycerides
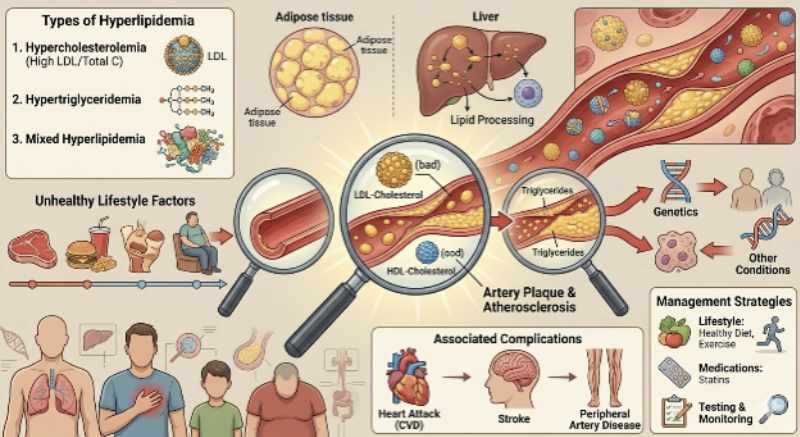
Types of dyslipidemia are classified based on the composition of these values; for example, distinctions are often made among the patterns of ‘predominantly hypercholesterolemia,’ ‘predominantly hypertriglyceridemia,’ and ‘mixed’.
To be continued


